Eczema doesn't mean asthma is inevitable! This PAI article decodes the "variable trajectories" of allergies.
2026.01.17 | 133
In the pediatric clinic, the most common question parents ask is: "Doctor, my child has eczema now. Will they really develop asthma later?" For a long time, the medical community has held a classic theory—the "Atopic March." It describes the process of childhood allergies like climbing a staircase: starting with eczema in infancy, gradually progressing to food allergies, and then to asthma and allergic rhinitis in school age. In 2025, a new in-depth review was published in the international authoritative journal Pediatric Allergy Immunology. Authored by multiple experts from the European Academy of Allergology and Clinical Immunology (EAACI), the article points out: Allergies are not a one-way street, but a variable "multi-trajectory journey."
I. Shaking Conventional Wisdom: Not Every Child Follows the "Script"
The latest global birth cohort studies confirm that the so-called "allergy staircase" is just one possibility. In fact, the progression of childhood allergic diseases shows "multi-trajectory" evolution: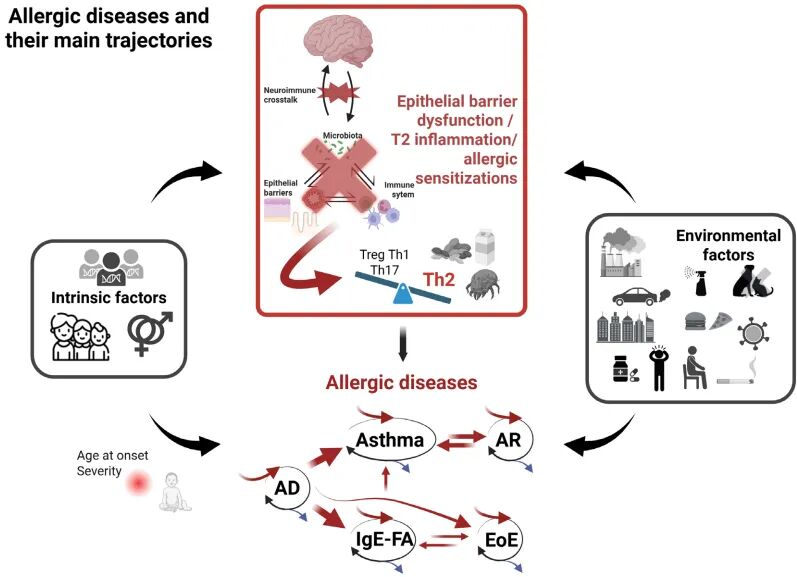
- "Transient" trajectory: Many children's eczema naturally resolves in early childhood, after which they remain problem-free. Possible mechanisms: Skin barrier maturation, establishment of immune tolerance.
- "Multiple coexisting" trajectory: This is the most concerning. Children do not develop one disease after another; instead, eczema, food allergies, asthma, and other symptoms occur simultaneously or alternately.
- "Atypical" trajectory: Some children skip eczema entirely, with food allergy or asthma as the first symptom. These children are at risk of being underestimated early in clinical care.
Each allergic child's future is uncertain. Recognizing the essence of "trajectory diversity" is the premise for precise prevention and treatment.
II. How to Predict a Child's "Allergic Endpoint"?
Since trajectories are variable, how can we predict whether a child will "recover" or progress to "severe disease"? As shown in the figure, the diversity of allergic trajectories stems from the interaction of genetic, environmental, and immune mechanisms.
- Genetic Background and Gene Polymorphism
Genetics is the underlying logic of an individual's allergic constitution. Family history of allergies not only determines the probability of onset, but specific gene expressions also predict disease progression. - Epithelial Barrier Function Status
- Skin barrier: The severity and duration of early eczema, as well as increased transepidermal water loss, indicate impaired barrier function, increasing the risk of sensitization through the skin.
- Intestinal/Respiratory barrier: Increased intestinal permeability and respiratory mucosal inflammation are also portals for allergen invasion.
- Early Microbiome Characteristics
- Gut microbiota imbalance: Lack of beneficial bacteria like bifidobacteria and faecalibacteria in infancy, or over-colonization by potentially harmful bacteria like Staphylococcus aureus, is closely related to the occurrence and development of allergic diseases.
- Allergen Sensitization Status: IgE Levels and Dynamic Changes
Allergen sensitization status, especially the level and dynamic changes of allergen-specific IgE, is considered a key biomarker for assessing disease risk and predicting trajectory evolution. This suggests that in allergen testing, precise quantitative analysis is far more clinically valuable than simple "positive/negative" judgments.
III. Precise Quantitative Testing: The "Beidou Navigation" of Allergy Management
- Identify "Initiating Factors" and Block Chain Reactions
Research has found that early sensitization to specific components (e.g., dust mites, cat dander) can highly predict future risk of respiratory allergies. Precise quantitative detection can capture subtle numerical changes, precisely identifying the "culprit" while symptoms are still mild, and block its evolution toward a "multiple coexisting" trajectory through early intervention. - Distinguish "Pseudo-improvement" from "True Remission"
Often, when a child's skin is no longer itchy or they are no longer wheezing, it doesn't mean the allergy is gone. If IgE quantitative values remain high, it indicates the immune system is still in a "high alert" state. Once medication is stopped or triggers are encountered, the condition will rapidly rebound. Dynamic monitoring of numerical changes is the only scientific basis for doctors to judge whether to reduce or discontinue medication. - Assess "Tolerance Thresholds" and Avoid Shock Risks
For children with food allergies, IgE absolute values directly relate to the severity of reactions. Through precise quantification, doctors can more safely assess whether a child can begin to try introducing certain foods, avoiding the risk of anaphylactic shock from blind trial eating.
IV. Expert Recommendations: From "Symptom Treatment" to "Precise Intervention"
The future of allergy management is moving toward "precision medicine":
- Early screening: Perform IgE quantitative testing during the eczema stage to assess future risk.
- Track trends: Don't test just once; schedule regular follow-ups to observe numerical trajectories.
- Choose precision: Select quantitative detection systems with high sensitivity and wide linear ranges. Small numerical fluctuations may significantly impact the entire treatment plan formulation.
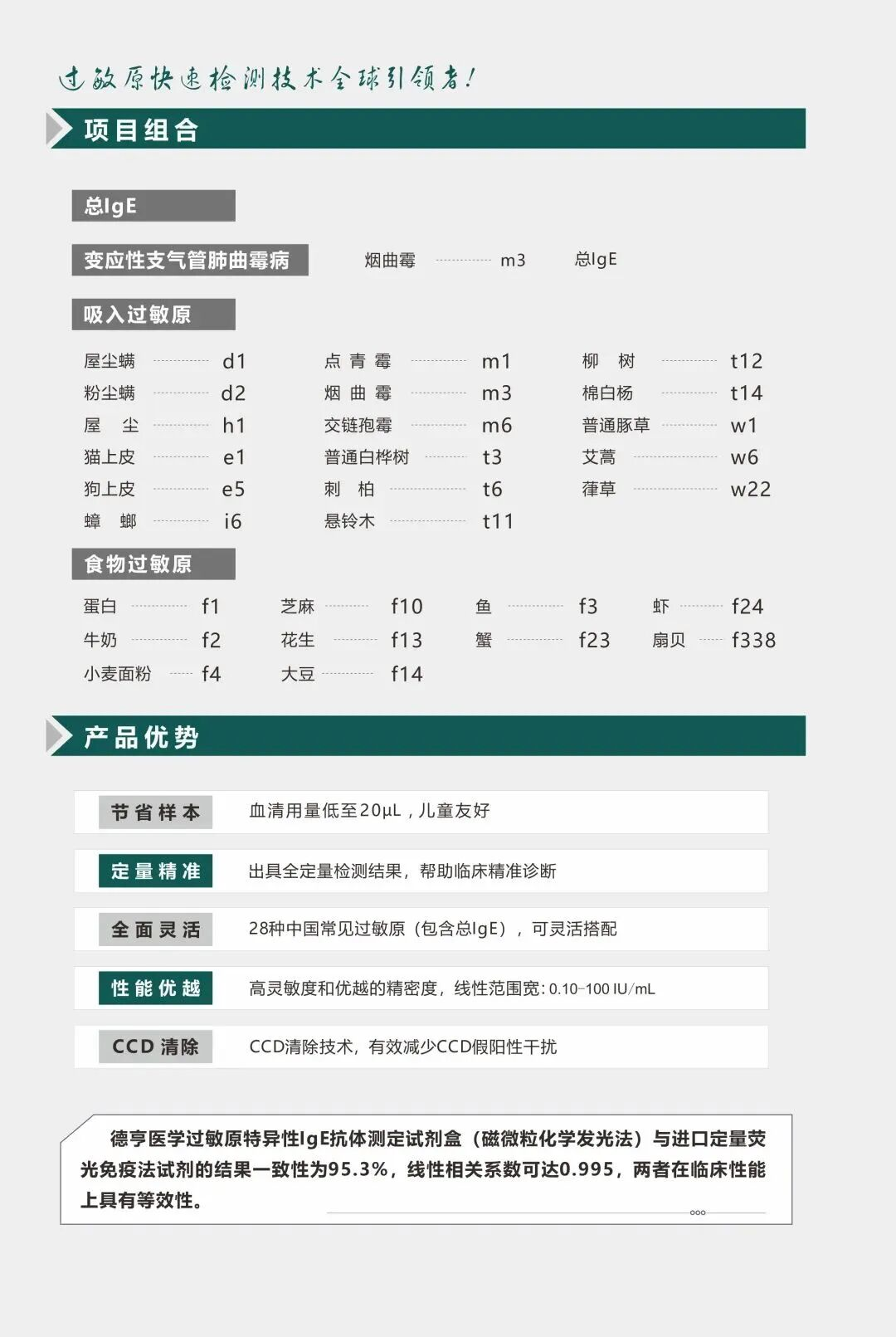
References: Kalb B, et al. Trajectories of allergic diseases in children: Destination unknown? Pediatric Allergy Immunology. 2025. Deheng Medical Allergen-specific IgE Antibody Assay (Quantum Dot Immunofluorescence), Deheng Medical Food-specific IgG Antibody Detection (Quantum Dot Immunofluorescence), Deheng Medical Allergen-specific IgE Antibody Assay (Magnetic Particle Chemiluminescence).